Breast cancer
Breast cancer - Female, 68 years, ductal carcinoma, grade 1, Elston-Ellis score 4 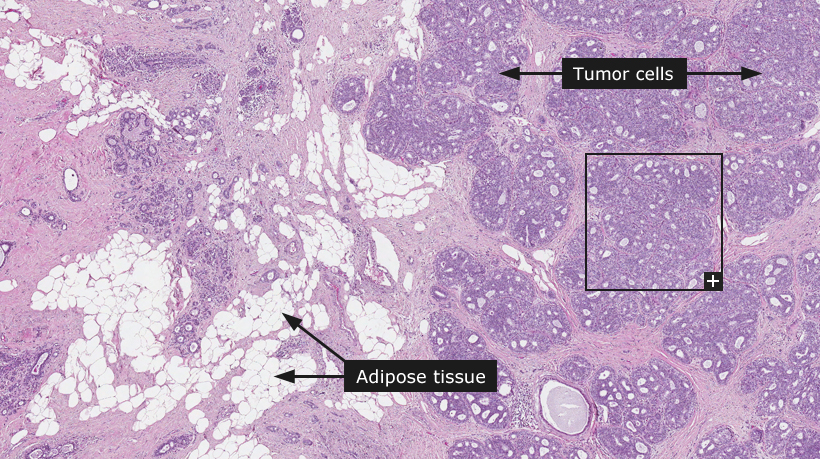
Breast cancer
Breast cancer forms in tissues of the breast, usually the ducts (tubes that carry milk to the nipple) and lobules (glands where the milk is produced). It occurs in both men and women, although male breast cancer is exceedingly rare. The age-adjusted incidence rate for breast cancer is 124 per 100,000 women per year, with the highest incidence found in women of Caucasian ethnical background and lower incidence rates in Asians and Hispanics. Breast cancer is the most common non-skin cancer and the second leading cause of cancer-related death in women in the western world. Although the rate of breast cancer diagnosis increased during the 1990's, it has decreased since the year 2000 and the overall breast cancer death rate has dropped steadily in the western world. The incidence in Asia is believed to be increasing although accurate statistics are unavailable.
The majority of breast cancers occur sporadically, but for 5-10% of patients there is a hereditary component. The most well known genes associated with increased breast cancer risk are BRCA1 and BRCA2. Women with an abnormal BRCA1 or BRCA2 gene experience up to a 60% risk to develop breast cancer by the age of 90.
Breast cancers are staged based on the presence of local and/or distant spread. Localized, disease (Stage I) comprises approximately 60% of cases, while in about 5% the cancer has spread to distant organs such as liver and bone (Stage IV). Approximately 35% are Stage II or III, indicating tumor spread to regional lymph nodes.
In a large proportion of breast cancer, precursor lesions such as intraductal carcinoma are present adjacent to the invasive component of the tumor. Such regions of non-invasive cancer are denoted as cancer in situ and are important to recognize in the diagnostic procedure. Breast cancer is broadly classified as ductal or lobular cancers depending on morphology and presumed site of origin. All breast cancers may be differentiated histologically into three grades utilizing the Nottingham Grading System (NGS), also termed the Elston-Ellis grading system, by evaluating three tumor parameters. Parameters evaluated in this system are (i) extent of tubular differentiation, (ii) nuclear pleomorphism and (iii) mitotic activity assessed by counting mitotic figures in ten high power fields. Each parameter is given a score of 1 to 3 and the score of all three components are added together to a final score e.g. 1+1+1=3. The lowest final scores of 3, 4 and 5 represent well-differentiated tumors (Grade I) associated with better survival. The highest possible score is 9 (3+3+3=9) reflecting a poorly differentiated (Grade III) tumor associated with poor overall survival.
Immunohistochemistry is used routinely on all breast cancers to gain important information about the prognosis as well as for predicting response to specific anti-cancer therapies. The most commonly used antibodies include antibodies detecting the estrogen a receptor (ER, ESR1), progesterone receptor (PR, PGR), HER-2 (ERBB2) and the proliferation marker Ki-67 (MKI67). The tumor stage and grade, as well as results from immunohistochemistry, are used to personalize treatment options.
Normal tissue: Breast
|




























