Skin cancer
Male, 26 years, moderately differentiated squamous cell carcinoma 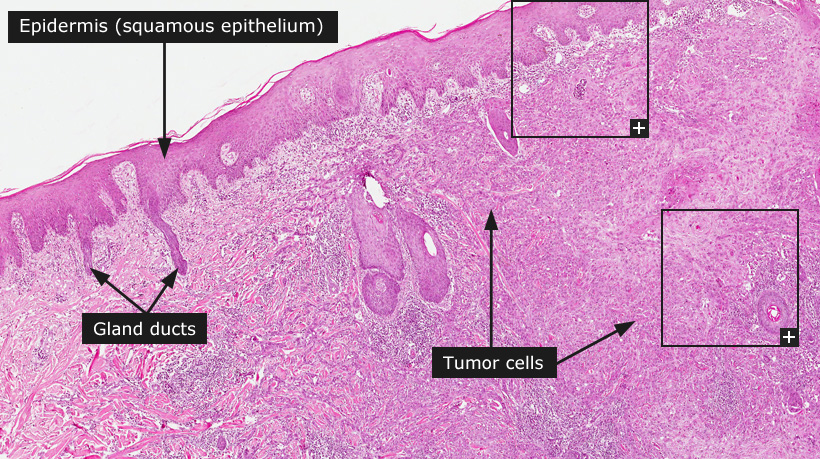
Skin cancer
Skin cancer can be divided into melanoma (see separate text and examples) and non-melanoma skin cancer. Non-melanoma skin cancer consists of two main subtypes, basal cell carcinoma and squamous cell carcinoma. Both these types of cancer are common and ultraviolet radiation from the sun is considered as the main etiological factor. The primary treatment is surgical removal of the tumor, which in most cases is sufficient for cure.
Basal cell carcinoma is the most common form of cancer in Caucasians and is rare in populations with more pigmented types of skin. The precise incidence of basal cell cancer is unclear, as this tumor type has not been included in the common cancer registries. It has been suggested that the incidence of basal cell cancer outnumbers all other forms of cancer taken together. Recreational sun exposure in young adulthood is considered as an important risk factor.
Basal cell cancers grow in hair bearing skin and the most common location is facial skin. Alike other epithelial malignancies, basal cell cancer exhibits invasive growth, but only in exceptional and rare cases does this type of tumor appear to develop metastases and thus prognosis is excellent.
Basal cell cancer develops without any known precursor stages and tumor progression is not a feature. The progenitor cell for basal cell cancer is believed to reside within the niche of hair follicle stem cells. Classification of basal cell cancer is descriptive and four major subtypes can be identified based on the microscopical growth pattern: (i) superficial, (ii) solid/nodular, (iii) intermediate and (iv) sclerosing type. The sclerosing type shows the most aggressive growth pattern with diffuse invasive growth of small strands of tumor cells surrounded by a specific fibroblastic tumor stroma. The common histopathological features of basal cell cancer include undifferentiated tumor cells (basal cell-like) with a pallisading arrangment of nuclei in the periphery of tumor nests. The tumor is often seen as connected to the epidermis and surrounding the tumor there is often a specialized loose connective tissue stroma rich in fibroblasts and collagen.
Squamous cell cancer of the skin is a common form of human cancer, mainly in Caucasian populations, and is most frequently located in facial skin and skin subjected to chronic sun exposure. The main risk factor for cutaneous squamous cell cancer is accumulated exposure to ultraviolet radiation from the sun. Squamous cell cancer in skin typically develops through precursor stages. A common precursor lesion is actinic keratosis, which is defined as epidermal dysplasia without invasive growth in combination with signs of ultraviolet damage in the dermis (solar elastosis). Squamous cell cancer in the skin can progress to poorly differentiated cancer and eventually develop metastases. Development of metastases is uncommon for squamous cell cancer of ordinary skin. However, squamous cell cancer that develops in skin adjacent to mucosal surfaces, e.g. lips and peri-genital/anal skin can often be more aggressive and metastasize to regional lymph nodes.
The histopathological features of cutaneous squamous cell cancer include growth of atypical cells with squamous differentiation into the dermis and deeper lying structures. The tumors can vary in degree of differentiation from well differentiated tumors with extensive keratinization to poorly differentiated tumors with severe cellular atypia and only hinted signs of squamous differentiation.
Normal tissue: Skin
|

















